A shot of truth about the flu shot
By Dr.Poonam Balaji
Vaccines are perhaps one of the greatest known inventions of science. We realize the significance of vaccination now more than ever as we desperately seek for a vaccination for the corona virus to stop the global pandemic.

{kind=link}
Vaccines
The first vaccine was discovered by Edward Jenner in 1798, against small pox. Since the discovery of the small pox vaccine a number of vaccines have now become available against several deadly diseases such as polio, tuberculosis, measles, rubella, diphtheria etc. Thanks to vaccines some of the most deadly diseases such as polio1 and small pox2 are now almost eradicated from this planet.
Vaccines train the human immune system to recognize and fight pathogens such as bacteria and viruses without exposing the body to the disease symptoms. Vaccines are made of inactivated/ dead or weakened form of the pathogens (antigens). They can’t cause an infection, but when the immune system is exposed to them, it still sees them as a foreign particle and produces antibodies in response.
A primary goal of vaccination is generation of antibodies for a sustained period of time. Months after vaccination the antibody levels peak, followed by a decline to a plateau level which may then be maintained for decades with minimal decline. Research has shown that these plateau antibody levels are maintained by specialized non dividing cells in our immune system residing in the bone marrow called bone marrow plasma cells (BMPC)3. BMPC have the potential to survive indefinitely in both mice and humans4 while also continuously secreting antibodies. Further, total and antigen-specific serum antibody levels correlate closely with BMPC numbers in humans.
Why do you need to get a flu shot every year?
{kind=link}
The best vaccines- measles, rubella, and diphtheria5– are the ones which offer 100% protection and last for life and you only need to take them once or twice (booster doses). Flu vaccines however are another story.
Research published in the journal Science by Rafi Ahmed and colleagues 6 from Emory University, Atlanta looked at BMPC to understand the sustainability problem of the flu shot. The antibody levels following vaccination depends on the number of BMPC7. The more the BMPC numbers greater the concentration of the serum antibody.
In case of the flu vaccine, antibody levels and protection conferred decline rapidly following vaccination, suggesting that the vaccine may fail to elicit BMPC, or that these BMPC fail to become long-lived. To investigate this the authors in this study examined the bone marrow and blood of 53 volunteers aged between 20 and 45 years old in the weeks and months before and after they received their flu shots. The unique aspect of this study is drawing the bone marrow from individuals which is a challenging and painful procedure that involves piercing the pelvic bone with a special needle.
28 days after flu vaccination the human influenza specific BMPC are generated and their numbers were significantly higher in these individuals then before the flu shot. But after 1 year, the new cells were virtually gone which explains why we would need to get a flu shot every year! According to the authors – “Several steps are required for a BMPC to become a long-lived plasma cell: the cell must reach the appropriate survival niche and successfully compete for space there, and the cell must undergo changes in gene expression and metabolism that promote longevity. Thus, our data suggests that most vaccine-induced BMPC fail at one or more of these steps.”
One of the suggestions made by the authors for improving the durability and efficacy of the flu shot by increasing the influenza specific BMPC numbers, is by utilizing adjuvants in the flu vaccine.
Adjuvants8 are ingredients (chemicals) added to vaccines to boost their immune response. In other words adjuvants make vaccines work better. Adjuvants have been safely used in vaccines for decades. In fact, the original flu vaccination did have an adjuvant.
A few modifications have been made to the flu vaccination over the past several decades. 1) The first influenza vaccines, developed in the 1940s, contained killed flu viruses mixed with a water-in-oil emulsion called incomplete Freund’s adjuvant. But the adjuvant was dropped in subsequent vaccines as it caused ulcers at the injection site. 2) Researchers have also stopped using the entire inactivate/ killed virus in the flu vaccine, replacing it with only the surface proteins from the virus to mitigate unwanted side effects. These flu vaccines are being used widely nowadays due to fewer side effects but at the cost of long term immunity.
Over the past decade a number of adjuvants9 are being deemed safe to be included in the flu vaccine and it would be interesting to see if they enhance the BMPC response of the flu shot. More detailed research is needed in this area. Until then the truth of the flu shot is that you need to keep getting one every year!
References:
- Soucheray, S. World Polio Day: Wild poliovirus type 3 declared eradicated. https://www.cidrap.umn.edu/news-perspective/2019/10/world-polio-day-wild-poliovirus-type-3-declared-eradicated.
- World Health Organization. Frequently asked questions and answers on smallpox. https://www.who.int/csr/disease/smallpox/faq/en/#:~:text=Smallpox was fatal in up,was in Somalia in 1977.
- Pioli, P. D. Plasma Cells, the Next Generation: Beyond Antibody Secretion. https://www.frontiersin.org/articles/10.3389/fimmu.2019.02768/full.
- Chernova, I. et al. Lasting Antibody Responses Are Mediated by a Combination of Newly Formed and Established Bone Marrow Plasma Cells Drawn from Clonally Distinct Precursors. J. Immunol. 193, 4971–4979 (2014).
- Cohen, J. How long do vaccines last? The surprising answers may help protect people longer. https://www.sciencemag.org/news/2019/04/how-long-do-vaccines-last-surprising-answers-may-help-protect-people-longer.
- Davis, C. W. et al. Influenza vaccine–induced human bone marrow plasma cells decline within a year after vaccination. Science (80-. ). 20, eaaz8432 (2020).
- Turesson, I. Distribution of Immunoglobulin‐containing Cells in Human Bone Marrow and Lymphoid Tissues. Acta Med. Scand. 199, 293–304 (1976).
- Control, C. for D. Adjuvants and Vaccines. https://www.cdc.gov/vaccinesafety/concerns/adjuvants.html#:~:text=What is an adjuvant and,adjuvants help vaccines work better.
- Tregoning, J. S., Russell, R. F. & Kinnear, E. Adjuvanted in fl uenza vaccines. 14, 550–564 (2018).
COVID-19 research update
An update on COVID-19 research
Several publications over the past week have started to focus on the differences observed in COVID-19 patients. While it is widely reported that COVID-19 has “specific” populations that it affects more severely than others (men, elderly, those with other health morbidities) it isn’t exactly known why these differences exist.
Research groups across the world have been investigating these disparities. Dr. Balaji has shared research from Wang, Hansen and colleagues who suggest that the composition of cell membranes, which varies throughout a person’s life, may be responsible for increased infection and possibly disease severity. Other groups have been examining other aspects of these patients to try to determine if there are additional differences that may explain these disparities and provide diagnostic and therapeutic opportunities.

Increased cases of COVID-19 in Puerto Rico over the past two weeks (7-12-2020 through 7-26-2020). This graph presents the percent increase over the past two weeks and represents the cumulative/total number of cases. Each municipality is colored with the median age of the population. Data from JHU-CSSE.
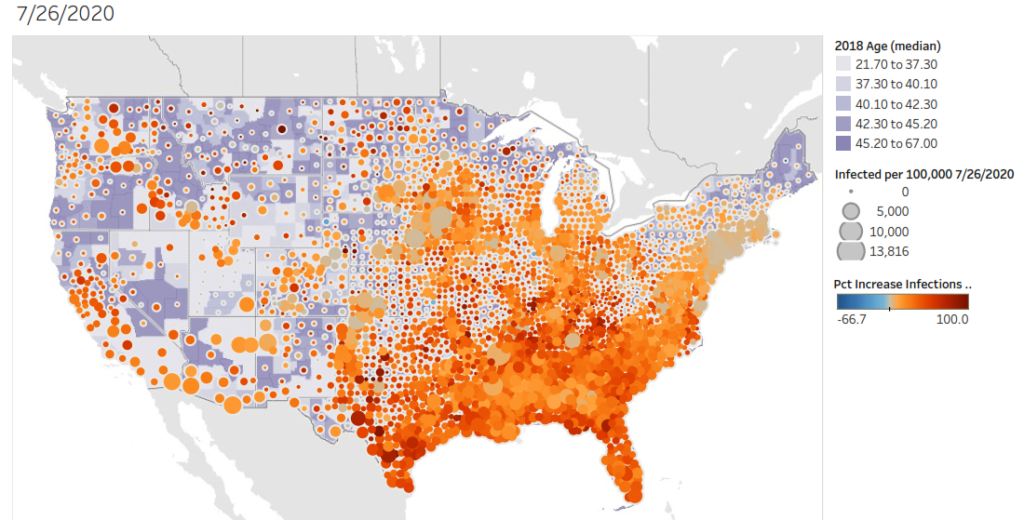
Increased cases of COVID-19 in the United States over the past two weeks (7-12-2020 through 7-26-2020). This graph presents the percent increase over the past two weeks and represents the cumulative/total number of cases. Each county is colored with the median age of the population. Data from JHU-CSSE .
COVID-19 Review1
COVID-19 is a disease caused by infection with the SARS-CoV2 virus. Entry into the cell allows the virus to replicate and infect other cells, while severely compromising cellular, tissue and organ function. Recognition of infection by the immune system mobilizes a robust response against the infection, at least initially.
In severe and critical cases of COVID-19, which have the highest risk or fatality and complications, there is mounting evidence for lymphopenia (T and B cell depletion) and for infiltration from myeloid cells. Myeloid cells are a type of immune cell involved in innate immunity and not tailored for response to viruses.
It appears that an initial/early response gives way to a late/mature response where adaptive immune cells are either ineffective or absent. The inflammation caused in the early stages of the response appears to impair expansion of T-cells and leads to the apoptosis of those cells that are present.
Identifying T-cell populations in patients with COVID-192
In a recent study published in the online pre-print bioRxiv.org Mathew and colleagues examined 125 patients and profiled them using deep immune profiling through flow-cytometry. Most of the patients examined are similar to a typical severe COVID-19 patient, being male and around 60 years of age. The patients were skewed towards African-American (68%) with cardiovascular risk factors present in 83%.
About one fifth of patients (18%) were immune suppressed for reasons not related to COVID-19. Most patients had been treated for their COVID-19 diagnosis (45% hydroxychloroquine, 31% with steroids and 29% with remdesivir). These characteristics may impact the results of the groups research and they will need to be controlled in future research.
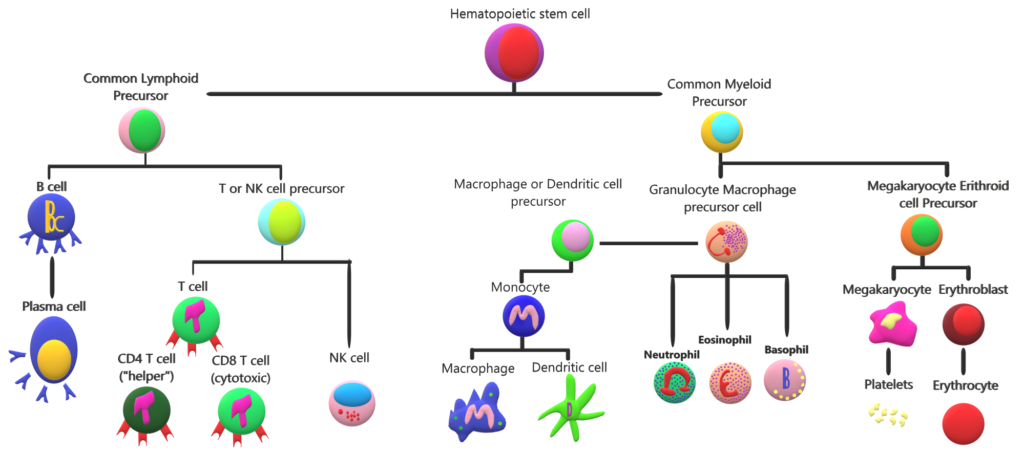
A hematopoietic cell “family tree”. Hematopoietic cells mediate systemic functions from oxygenation to damage repair and pathogen removal. In this graph we can see that T cells are related to myeloid cells. These two cell types carry out different immune functions. The presence or absence of a sub-set of cells results in the variety of responses that our immune system is capable of carrying out. In COVID-19 the absence or “exhaustion” of T cells results in a weak immune response that may lead to damage of surrounding tissue.
Most patients were enrolled nine days after symptom development. Markers of inflammation immune response, blood clotting and cell death were elevated in most patients (>75%). The inflammatory cytokine IL-6 was elevated in 88% of patients.
The purpose of the experiment was to compare patients with active COVID-19 to those that have either never had COVID-19 and a group that had recovered (control groups). The researchers found differences between these groups that suggest three distinct COVID-19 patient populations based on T cell response.
The research group confirmed the known clinical symptom of lymphopenia (B and T-cells decrease) in their COVID-19 patients. While total white blood cell counts were elevated they found that B or T cells were not increased. This is because the elevated cells belong to the myeloid type of immune cell.
The researchers identified three types of patients based on the presence of proteins and clinical outcomes. Disparities or T cell diversity may have an impact on regulation of the immune response. This finding may help identify predictors of COVID-19 progression and survival.
The observed reduction was highest in CD8 T cells, which are important regulators of viral infection. T cells are broadly categorized into two groups, CD8 and CD4, based on their functions. CD4 T-cells are called “helper” cells and they mostly act as organizers by stimulating other immune cells and ensuring proper actions to restrict damage to surrounding tissue. This is the type of T cell that is deficient in patients with HIV. CD8 T-cell are sometimes called “killer” cells because they produce strong signals to infected cells to initiate programmed death of an infected cell.
Examination of the proteins present on cell membrane through the use of flow cytometry. The researchers identified three types of patients based on the presence of these proteins and a patient’s clinical outcome. Some patients had a profile of high activation in their CD4 T cells, with very high, possibly exhausted CD8 cells. A second group had high CD8 activity, but low CD4 activity. Lastly, there was a group of about 20% of patients that had no T cell response. Researchers don’t know the reason for these differences and additional research is necessary to fully understand the impact of these differences on each patient’s prognosis, survival and long term recovery.
Disparities or T cell diversity may have an impact on regulation of the immune response (CD4 T cells), myeloid cell recruitment (CD4 T cells), induction of cell death in infected cells (CD8 T cells) and antibody production (CD4 T cells). The finding of these differences between patients may help identify predictors of COVID-19 progression and survival. Our understanding of the differences between these groups may aid medical personnel in reducing mortality, increasing recovery and enhancing long-term prognosis of patients in each group.
Symptoms and differences in affected populations
A study of almost 45,000 people in China found that 81% of people get a mild form of the disease with fever, cough, sore throat and other symptoms of a cold. Fourteen percent of those infected get a severe form of the disease. These patients show difficulty breathing and fatigue. Finally, there are about 5% of patients that present a critical, life-threatning form of COVID-19 with respiratory and other organ failure.
While 25% of people infected with COVID-19 have co-morbidities, more than 60% of those in hospitals have co-morbidities. This disparity and suggests that co-morbidities exacerbate COVID-19. Another observed disparity comes from age when infected. Children (< 18 years of age) typically have milder symptoms that are limited to the upper respiratory tract and they rarely require hospitalization. In very rare circumstances a multisystem inflammatory syndrome has been reported in children of European descent.
Looking at populations with prior exposures to other viruses3
Another recent publication examined mounting evidence of COVID-19 patients with particular interest in their prior infections. Kadambari and colleagues suggest that previous infection with Cytomegalovirus (CMV), a common virus that infects large percentages of the population may explain some of the differences observed based on age. In people with a healthy immune system, the infection rarely causes problems.
The research group points out that as we get older we lose an important organizer of the immune response, T cells. As we age, our immune system becomes less effective and as a consequence older adults with a CMV infection may have complications. The CMV virus may suppress the immune system even further than the natural age-related decline.
In people previously infected and recovered from CMV the percentage of T-cells dedicated to fighting off virus is higher than in those that have never been exposed. The focus on fighting off the CMV leads to a lack of T cell diversity. This is compounded with a normal decline in T cell diversity as we age.
Because most T cells are singularly focused on fighting off CMV, the immune response to new antigens and pathogens is curtailed, leading to the cytokine storm observed in some patients. This T cell dysregulation, along with co-morbidities found in elderly patients, may explain the increased severity and mortality observed in the elderly.
Immune cells and development of severe COVID-19
Autopsies of COVID-19 victim’s reveals macrophages and mononuclear cells, some of the myeloid cells mentioned above, occupying the airspaces of the lung along with severe inflammation of the surrounding vascular tissue. Alveolar spaces, the tiny pockets of our lungs where gas exchange occurs are filled with liquid which starts to form a membrane indicating a condition called Acute Respiratory Distress Syndrome (ARDS).
In patients with ARDS the likelihood of dying is greatly increased and in survivors it causes lung tissue scaring and blood clots. It also predisposes survivors to infections and psychological symptoms. In some cases there is increased coagulation and complications with thrombosis, complicated with viral sepsis, which can lead to organ or multi-organ failure and death.
SARS-CoV2 transmission
Transmission mostly occurs through respiratory droplets generated when speaking with someone in close-quarters. Infected individuals may remain without symptoms for up to 11 days, although most people develop symptoms during the first week. Most infections are thought to be transmitted from infected individuals that show no symptoms. While spread from asymptomatic is likely very uncommon, although care should be taken since there is no way to distinguish asymptomatic individuals from pre-symptomatic individuals.
For these reasons people are asked to physically distance when outside of their homes. In situations where an individual may come in contact with another person, masks are suggested to reduce the emission or receipt of respiratory droplets. Outside of laboratories there is no evidence that the virus can remain in the air for a long time and cause infection through aerosols.
While the virus is able to survive on non-permeable surfaces, such as stainless steel or plastics for up to four days, there is likely minimal risk of contagion from surfaces. If you touch a surface outside your home, use soap and water (if available) to wash your hands before touching your face or alternatively use hand sanitizer. Avoid touching your face while out in public.
Treatment
More than 75% of those hospitalized with COVID-19 require oxygen. For some of these individuals positioning and muscle relaxants can help improve breathing. Other patients may require oxygenation and intubation to provide enough oxygen to survive.
Some patients may be treated with anti-viral drugs, although initial results indicate that hydroxychloroquine and lopinavir show no improvement over standard of care. Initial results of success by using convalescent plasma have also been tempered by reports of larger cohorts where no improvement is observed in severe and critical patients receiving this plasma.
Immunomodulatory drugs that reduce inflammatory proteins like IL-6 may be effective at controlling symptoms of unregulated inflammation and decreasing tissue and organ damage. Some studies suggest that immune damage to self could be controlled through the use of immune suppressant steroids such as dexamethasone and methylprednisolone to reduce the chance of ARDS. The benefits of using these medications must be weighed by medical personnel with access to a patients history and against the risk of secondary infections.
It is also important to remember that critically ill patients that recover continue to need medical assistance, in some cases for years. Survival from sepsis leads to long term physical disability, cognitive impairment and increased vulnerability to infection.
As we continue to learn more about SARS-CoV2 infection, opportunities to improve patient outcomes will increase. The shifting focus will be especially important to the recovery once the pandemic is under control and we are able to turn our attention to the needs of those recovering from the infection. The mental health toll of the strategies chosen to deal with the pandemic, the effects of the infection on people’s lungs and vascular tissue, along with possible cognitive impairment following COVID-19 will require novel strategies and will continue to impact our society for a long time.
References:
- Wiersinga, W. J., Rhodes, A., Cheng, A. C., Peacock, S. J. & Prescott, H. C. Pathophysiology, Transmission, Diagnosis, and Treatment of Coronavirus Disease 2019 (COVID-19): A Review. Jama 2019, 1–13 (2020).
- Mathew, D. et al. Deep immune profiling of COVID-19 patients reveals patient heterogeneity and distinct immunotypes with implications for therapeutic interventions. bioRxiv Prepr. Serv. Biol. 8511, 1–29 (2020).
- Kadambari, S., Klenerman, P. & Pollard, A. J. Why the elderly appear to be more severely affected by COVID-19: The potential role of immunosenescence and CMV. Rev. Med. Virol. 1–5 (2020) doi:10.1002/rmv.2144.
Is there a link between cholesterol and COVID-19?
Is there a link between cholesterol and COVID-19?
By Dr. Poonam Balaji
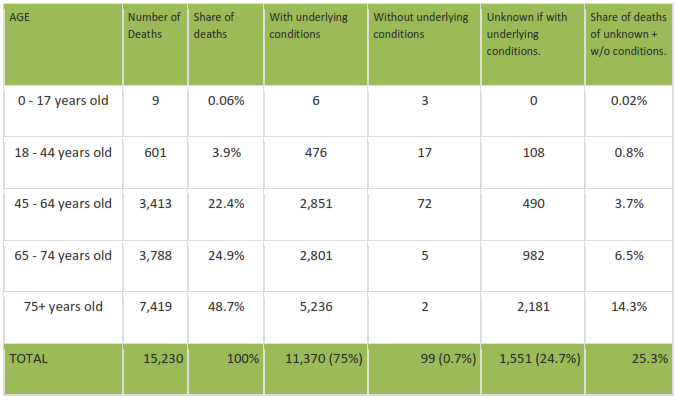
The coronavirus SARS-CoV2 and its associated disease, COVID-19, is particularly devastating in the elderly. COVID-19 is especially deadly in those with other co-morbidities such as heart disease, hypertension or diabetes. As shown in the table below (New York City data) most of deaths due to COVID-19 happen in people over 65 years of age accounting for nearly 75% of deaths1.
COVID-19 among young people
A small silver lining, to the COVID-19 pandemic is that children are either mostly asymptomatic or show very mild symptoms. Children also do not easily maintain physical distance or naturally think about hand-washing. They are also still learning to cover their mouths when they cough or sneeze. Since children are in contact with older adults and rarely show symptoms the outbreak is much harder to control.
Interestingly, during the previous SARS outbreak in 2002-2003 (which killed 774 people and infected more than 8,000)2 a similar trend was observed where no deaths were observed in children 12 years and younger. Children somehow seemed to have been protected. There were only 80 laboratory-confirmed cases and 55 probable or suspected cases of SARS in children. Scientists still don’t understand the reason for this disparity in the lethality of the virus in adults’ compared to kids.
Understanding the cause and mechanism of protection against viruses such as SARS in kids could possibly be the key to the tackling not only the current pandemic but also to prevent future outbreaks.
Age of COVID-19 Deaths in NYC2
How does SARS-CoV2 enter the cell?
For over 100 years the scientific community hasn’t reached a consensus on whether viruses are living or non-living. One of the most fundamental requirements of a living organism is the ability to reproduce. Viruses are microscopic infectious particles which can’t replicate on their own. They can replicate when they enter living cells. Therefore, viruses are thought of as being in the gray area between living and nonliving. Can you believe something this tiny and not even alive on its own can cause such havoc?
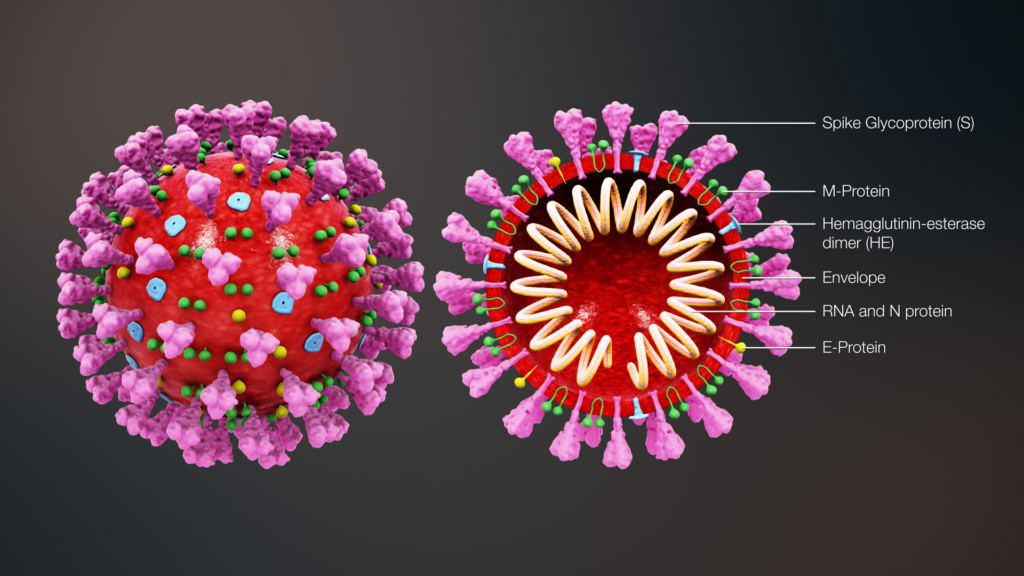
The process of viral replication begins with entry. For the coronavirus that process is initiated by the spike protein (S protein) which are the little protrusions sitting on the top of the virus. Unsurprisingly, the most popular photo around these days shows these protein protrusions. The protein (receptor) in living cells which aids the viral entry is called angiotensin converting enzyme 2 (ACE2). Binding of the spike protein (key) on the SARS-CoV2 virus to the ACE2 protein (lock) on the host cells, sort of like a key being inserted into a lock which enables viral infection by SARS-CoV1 4 and SARS-CoV2 5.
What is ACE-2?
ACE2 is expressed in the airways, lung, heart, intestines, kidneys and blood vessels. This enzyme is a critical component of a system that regulates blood pressure, fluid, and mineral balance in the body. It also plays an important role in wound healing and inflammation. ACE2 appears to be the gateway for the entry of SARS-CoV2 into the body via the nostrils, mouth, lungs and other organs. Therefore, it seems logical to ask whether the quantity of this receptor in the body has anything to do with the severity of the disease in adults.
If only science were that simple! As data has continued to be generated, conflicting and often paradoxical data about the levels of ACE2 are arising from research around the world. Initially, it was shown that the level of ACE2 is lowest in children which could explain their low rates of infection6, and being mildly affected by the disease. However, more recent data published to the pre-print repository BioRxiv indicates that the level of ACE2 is actually higher in children than in the adults 7. So this makes this story a bit more complicated and forces us to look for better explanations.
Does cholesterol have a role in COVID-19 infection?
In a recent pre-print article in bioRxiv scientists from The Scripps Institute in Florida suggest that cholesterol might play a role in age related COVID-19 infectivity and severity8. Cholesterol is found throughout the human body and is an important structural component of animal cell membranes. The accumulation of cholesterol in tissues however, increases with age and that contributes to morbidities such as atherosclerosis, increased blood pressure, stroke etc. Is there a link between age, cholesterol and COVID-19?
Coronaviruses are known to enter the cells by employing lipid rafts and via a process of endocytosis 9. Lipid rafts are microdomains found on the membranes (outer surfaces) of cells and is made up of chemicals called cholesterol and sphingolipids. These lipid rafts normally help in transporting substances required for normal cellular processes from the outside to the inside of the cells10. They can also act as a site of entry and assembly of pathogens such as the SARS-CoV viruses.
Scott B. Hansen and colleagues show that entry of SARS-CoV2 depends on the presence of cholesterol. Further, in the presence of high levels of cholesterol, the virus entry points on the cell membrane are both markedly increased in size and number. And reducing the amount of cholesterol in the cells has the opposite effect.
cholesterol levels and life styles
Cholesterol loading in cells significantly increases with aging and inflammation caused by smoking, atherosclerosis, diabetes, and other co-morbidities. This makes it more likely that SARS-CoV2 will infect more cells and cause significant damage to tissues of the elderly and people with co-morbidities. The authors suggest that cholesterol might be a key player in age related lethality due to COVID-19.
Another interesting point is that high levels of cholesterol cause an increase in trafficking of the ACE2 receptor to the viral entry point although this point also remains controversial 11. If ACE2 does traffic to lipid rafts it might increase docking of the S-protein. Cholesterol has also been shown to be important for efficient replication (division and reproduction) of enteroviruses and other the SARS-CoV virus. Whether the same holds true for SARS-CoV2 is yet to be determined.
Summary and recommendations
This study proposes a new model for age related lethality due to COVID-19 mediated by cholesterol. However there are a few caveats to consider. The bioRxiv website said it has been “receiving many new papers on coronavirus SARS-CoV-2.”Additionally they caution that “These are preliminary reports that have not been peer-reviewed,” and that “They should not be regarded as conclusive, guide clinical practice [or] health-related behavior, or be reported in news media as established information.”
The experiments in this paper were done in cell culture and not in animal models/humans. However, this does seem like a promising mechanism and could mean that there might be ways to look at treatment options for COVID-19, involving cholesterol lowering mechanisms.
Healthy diet and exercise are encouraged to lower cholesterol and could play a role not only in SARS-CoV2 infection, but for many other viral infections.
In summary, COVID-19 seems to be especially deadly in the old (>65 years old) and the vulnerable. Smoking, hypertension (which is prevalent in people over 40) and diabetes may lead to increase in inflammation associated with an increase in cholesterol and this could be one of the reasons for worse outcomes in these patients due to COVID-19.
Currently we are bang in the middle of this pandemic and we don’t have enough statistical evidence to make a direct correlation between cholesterol and death due to COVID-19. Once we are on the other side of this nightmare, there will be loads of demographic and statistical data which will help us better comprehend how each of these conditions correlate to worsening of coronavirus prognosis.
About Dr. Poonam Balaji:
I am a qualified scientist with a PhD in cardiovascular physiology and Molecular biology from The Ohio State University. I have over 15 years of experience in research and am passionate about everything science and medicine. Science communication is my new found interest. You can find more of my writing at https://cuppa.science.blog/.
References:
- Chen, T. et al. Clinical characteristics of 113 deceased patients with coronavirus disease 2019: Retrospective study. BMJ 368, (2020).
- Worldometer. Age of Coronavirus Deaths. https://www.worldometers.info/coronavirus/coronavirus-age-sex-demographics/ (2020).
- World Health Organization. Summary of probable SARS cases with onset of illness from 1 November 2002 to 31 July 2003. https://www.who.int/csr/sars/country/table2004_04_21/en/ (2003).
- Kuhn, J. H., Li, W., Choe, H. & Farzan, M. Angiotensin-converting enzyme 2: A functional receptor for SARS coronavirus. Cell. Mol. Life Sci. 61, 2738–2743 (2004).
- Wang, Q. et al. Structural and functional basis of SARS-CoV-2 entry by using human ACE2. Cell 1–11 (2020) doi:10.1016/j.cell.2020.03.045.
- Bunyavanich, S., Do, A. & Vicencio, A. Nasal Gene Expression of Angiotensin-Converting Enzyme 2 in Children and Adults. JAMA 323, 2427 (2020).
- Miguel E. Ortiz Bezara, Andrew Thurman, Alejandro A. Pezzulo, Mariah R. Leidinger, Julia A. Klesney-Tait, Philip H. Karp, Ping Tan, Christine Wohlford-Lenane, Paul B. McCray, Jr., D. K. M. Heterogeneous expression of the SARS-Coronavirus-2 receptor ACE2 in the human respiratory tract. (2020) doi:10.1101/2020.04.22.056127.
- Wang, H., Yuan, Z., Pavel, M. A. & Hansen, S. B. The role of high cholesterol in age-related COVID19 lethality. bioRxiv 15, 2020.05.09.086249 (2020).
- Ilnytska, O. et al. Enteroviruses harness the cellular endocytic machinery to remodel the host cell cholesterol landscape for effective viral replication. Cell Host Microbe 14, 281–293 (2013).
- Brown, D. A. Lipid Rafts. in Encyclopedia of Biological Chemistry 741–744 (Elsevier, 2013). doi:10.1016/B978-0-12-378630-2.00185-7.
- Tang, T., Bidon, M., Jaimes, J. A., Whittaker, G. R. & Daniel, S. Coronavirus membrane fusion mechanism offers as a potential target for antiviral development. Antiviral Res. 104792 (2020) doi:https://doi.org/10.1016/j.antiviral.2020.104792.
On pre-print publications
statement on use of pre-print publications
At Ourcellves.org we seek to participate in a community interested in the biological sciences and willing to engage in productive and enlightening conversations. Some of these conversations can be controversial and we welcome them. We have decided to share content accessed through pre-print repositories, but importantly want to echo the caveats of BioRxiv.org that “No endorsement of an article’s methods assumptions, conclusions or scientific quality… are implied…” At Ourcellves.org our use of data published on pre-print repositories does not imply endorsement. We do not suggest that the content shared has been validated or that it should be used to make decisions about health-care or public policy.
Science is a formalized methodology. It attempts to describe the natural world through observation, hypothesis testing, falsification and discussion. The results of this methodology are always subject to rigorous, informed and thoughtful debate. This is true for data, analysis and conclusions published in both traditional scientific journals and in new online pre-print repositories.There are benefits and drawbacks to publishing data on pre-print repositories.
Benefits
- Accessibility: A long standing difficulty within the scientific community is the dissemination of the knowledge produced by research at publically funded institutions. If the public funds the research, why should access to it be limited to individuals or institutions able or willing to pay exorbitant fees for access? The advent of newer policies such as “Open-access” have improved the situation, but not completely fixed it. Publication and accessing of research findings on “pre-print” repositories is currently free for anyone that is interested in the science. Still, there is no guarantee this will always be the case.
- Feedback: Research and findings will be examined, not only by peers within a scientists’ field, but theoretically by anyone with any background. Interesting conversations can be had with other experts about the impact of the science other branches of knowledge and in potential applications of the discoveries. The most widely cited repository for pre-prints, bioRxiv.org, specifically states that by posting to their site “authors are able to make their findings immediately available to the scientific community and receive feedback…” Clearly then the intent of the pre-print repositories is to improve the quality of science and not to provide “work-arounds” to rigorous study.
- Improvement in publishing rate: It takes a very long time to publish a paper. A 2016 article in Nature found that the median time from submission to publication is around 100 days. During this period the authors are not receiving meaningful feedback from peers. On the other hand, if their work is published in pre-print servers, authors get immediate feedback on the quality of their data, analysis and conclusions. They may even get feedback from experts outside of their fields leading to opportunities for collaboration and applications.
Drawbacks
-
- Lack of review: One of the major benefits of the peer-review process is that experts in the authors’ field of study are able to provide feedback without the need of extensive contextualization of the data, analysis or conclusions. Although it might be ultimately necessary to improve the quality of communication in the article, most expert peer-reviewers can complete the revision of the article without the need of extensive introductory statements or background information. It might be that pre-print publication improves the quality of science communication, while peer-reviewed publication improves the technical aspect of the research reported.
- Statements of conflict: The use of scientific communication to promote the use of a procedure or treatment is very old. As a matter of fact, most scientific articles carry the tag “Advertisement”. Still, the peer-review process can expose the interests, behind particular hypothesis and reveal the motivations behind analysis and conclusions. Statements on conflict of interest are not required in pre-print publications, although that may change.
- Increased speed of change: Keeping up with scientific literature is daunting. Currently, scientists searching through this vast literature can be confident that at least three experts have reviewed the publications before making them available. This in no way makes the published results a “law of nature”. It requires careful consideration before integrating it into your research design and conclusions. Still, it reduces the possibility of encountering published research with poor experimental designs, inappropriate measurements and lack of rigor while reaching conclusions.
Because we seek to explore the newest concepts and encourage discussion of both established and emerging ideas in biological sciences we will use pre-print publications as sources for some of the articles on our website. We will always include the caveats stated above about these publications.
Empathy and compassion
Empathy and compassion
Watching the slow moving pictures on the TV is making the humans sad. I try my best to make them feel better. And it works, at least for a little bit. I have recently heard a lot about anxiety and stress, and ways of reducing their impact.
Steven has recently been writing about compassion and how it is necessary for people to show compassion towards others and towards themselves. I want to write about compassion, because it is what I feel towards my humans. Also, understanding a situation, its basis and how we react allows us to cultivate effective coping mechanisms, help others and enhance our lives.
The world and our behaviors
Our central nervous system connects our bodies to our brain. Through our senses we collect information about our environment, send it back to our brains and process it into our responses. If while out for our walk Steven sees someone we like, he waves or says “Hello!” In turn they will wave and say “Hello!” if they like us. This pleasant exchange occurs because our brains recognize the other person and know they will not harm us. The results are very cool. I can’t say “Hello!”, but if I wag my tail at a human I know is carrying a treat, I get a milk-bone!
It is very confusing to talk about behaviors, especially our feelings for others. Therefore, I’m going to focus on two specific behaviors that arise when we see others experiencing pain or anguish.
These behaviors are the result of the same system that allows us to experience and analyze our environments. The same central nervous system that allows us to experience pain through hardship, is used to vicariously experience the anguish of others. We have the same cellular building blocks, the same cells and the communication between cells is dependent on the same neurotransmitters.
Empathy
Empathy, which a lot of people tend to confuse with compassion, is a natural feeling arising when we recognize that someone else is anguished or struggling. It allows us to share a frustrating and painful situation without having to experience it firsthand. Empathy balances our feelings and our thoughts towards another individual’s struggles. It is most likely a behavioral tool that aids with survival and it is an ancient behavior.
- Empathy requires that we recognize the other, the cause of the struggle and ourselves. By doing this, we can remove ourselves from the situation and lend assistance.
- It is important to know that empathy, does not automatically lead to helping someone, and that help is not always due to empathy. Empathy is about reducing the pain, anguish and stress of others. This feeling can be stressful and emotionally exhausting.
- Depending on the level of discomfort that others are experiencing, we might lend a hand, not because we want to improve others’ lives, but because we want them to stop bothering us.
We all have a natural need to keep ourselves safe and help others be safe. We also want to improve the lives of others and help them through difficult times. For example, rats in a laboratory that are trained to push a lever to receive food, refuse to push the lever if they see another rat experiencing pain as a consequence of pushing the lever. Rats prefer hunger to causing others pain!
Compassion
These feelings of empathy are then combined with a desire to improve the situations of others. Compassion is a complex set of behaviors built upon empathy.
- A hypothetical model of this behavior called the perception-action model (or PAM for short) suggests that seeing another undergo pain or anguish awakens feelings of empathy.
- We can intervene in a variety of ways to dampen these feelings. We might take pleasure in their suffering, we might ignore their pain or we may try to help.
- Deciding whether we should intervene and in which way, moves the decision-making upstairs. I mean this literally, it is higher parts of the brain carrying out these thoughts. Actively engaging the situation, we project the situation over our current emotional state, our state of mind, our past experiences and our ethnic/cultural framework.
- If we decide that we want to help, that we are not putting ourselves in danger and that we have a combination of the mindset, experience and the resources to help, we will lend a hand to improve the circumstances of the suffering other. This is compassion.
This is all easy and intuitive to understand. That is because of how ancient this behavioral mechanism is, and how we have adapted to it. We see these two behaviors in most mammals and birds, organisms that last shared a common ancestor over 300 million years ago.
A little girl recognizes the discomfort in the face of another girl and offers a toy to make her feel better!
We also see compassion and kindness in the attempts of primates and human babies to comfort an adult feigning discomfort. My personal favorite, dogs can detect the levels of a humans stress hormones and offer a good tail wag or face-lick! As you can imagine these behaviors are not meant to resolve a situation causing stress, but to offer my personal touch and experience to comforting. Humans offer each other words of kindness and comfort, I wag my tail and cuddle.
The basis of our behavior
These behaviors remain in our lives and are passed down to our offspring because they enhance our lives, and occur at different levels: physiological, personal and societies. There are actual neurological consequences to helping others, such as activation of parts of the brain involved in experiencing rewards. Activation of these areas make us feel energized, happy and relaxed.
When another suffering, imaging studies show that our brains respond in a similar way as if we were experiencing the pain. We call this mechanism empathic pain. Of course, because we are using the same cells and neurons to “feel” anothers pain. When we take medications to dull our pain or anxiety (such as acetaminophen or anxiolytic drugs) we become less receptive, understanding or helpful to the distress of others.
The benefits of compassion
More widely, empathy and compassion may signal that an individual might be a good partner, allowing us to forge strong and lasting relationships. It may also indicate that a partner may be a good parent, contributing to a feeling of security.
Compassion may reward us with positive feelings and better integration into family and social networks, but it is hard work. We must recognize the discomfort and separate ourselves from the situation. Then we must project the situation onto our memories and experiences and our current state of mind. Finally, we must come up with an appropriate response to the situation that will not only remove the pain and discomfort but provide life improvement, and this is just compassion towards others. Compassion with ourselves requires self-examination, knowledge of ourselves and the situation that requires cultivation and practice.
Get to it! Be compassionate! If you would like to know more, here are the resources I used:
- Goetz, 2010: Compassion as a separate behavior from empathy
- DeWaal, 2017: Mammals, behavior definitions, physiology and experiments
- Dowling, 2018: Compassion contrasted to emphatic concern and emotional exhaustion
Reading is hard work. Writing is hard work. Self-compassion is hard work. It’s much easier to be compassionate to others. Now, if you’ll excuse me, I have stressed humans whose faces need licking.
Mental health during the COVID-19 pandemic
COVID-19 is a respiratory disease caused by the SARS-CoV2 virus. While it can infect almost everybody, certain populations are at risk of developing severe/critical cases that endanger and even cost people their lives. The main reason for the lethality of this virus has not been determined. This is why people are asked to maintain physical distance and reduce the risk that a member of a vulnerable population becomes infected. This distancing also reduces the chance that hospitals or healthcare professionals become overwhelmed by a sudden increased in people with respiratory disease. Keep in mind, that along with new COVID-19 cases, there are other patients that these professionals encounter on a daily basis, since people haven’t stopped having accidents or other health complications.
These preventative measures (distancing) are likely to increase stress and the development of mental health disorders. While our bodies have “built-in” mechanisms for coping with short and long term stress, prolonged stressful situations may lead to:
- Anxiety: a generalized fear or feeling of dread about anticipated events. Anxiety has verifiable physiological responses and long term pathological consequences.
- Depression: a generalized lack of desire or interest in normal activities, feelings of hopelessness, changes in appetite and changes in sleep patterns.
- Post-traumatic stress disorder (PTSD): is characterized by distressing thoughts associated with a traumatic event, nightmares, changes in thoughts and moods and avoidance behavior. Those affected typically have to deal with long-term consequences of the traumatic situations that caused PTSD.
In this article you will find information about the effects of corona-virus infection on the human central nervous system. It will explore the effects of physical distancing and quarantining based on previous viral outbreaks. Finally, there will be recommendations regarding the best steps you can take to minimize the impact of physical distancing and/or isolation on your mental health.
Current approaches to control the COVID-19 pandemic
Physical distancing (often erroneously called social distancing) is the practice of maintaining at least six feet (two meters) of distance between each individual. This is to reduce the likelihood that respiratory droplets from an infected person may find their way into the respiratory track of a healthy person, infecting the healthy person 1.
A second strategy is to shelter in place and shares the same purpose as physical distancing. By remaining in a location for extended periods of time, individuals reduce their risk of coming into contact with surfaces that may contain virus or coming into contact with an individual that is infected. It also has the added benefit of reducing your likelihood of having an accident outside of your home.
People that have been infected with the virus and have recovered are asked to isolate from others while their bodies naturally get rid of the remaining virus. This is because the virus can remain in recovered individuals for many weeks 2. Even with common colds (which COVID-19 is not) this is good advice, because individuals can remain infectious days after they start to “feel better”.
People with COVID-19 and are hospitalized with respiratory distress often receive a combination of respiratory therapy and experimental medications meant to reduce the development of life-threatening complications. Various trials are currently underway to develop vaccinations which may provide long-term protection against the SARS-CoV2 virus.
All of these strategies are meant to “flatten the curve” by reducing the number of people that are infected with SARS-CoV2 and reduce the number of people requiring treatment in the hospital.
Effects of corona virus infection on the central nervous system
While we still don’t know much about how COVID-19 disease progression affects the central nervous system (CNS), there is some literature regarding infection by other corona viruses. The following section reviews the literature regarding the consequences of mental health in two previous outbreaks: SARS and MERS.
Viral infection results in increased production and release of inflammatory proteins called cytokines (Note: cytokines are a very complex protein class and sometimes have inflammatory roles, while they sometimes have anti-inflammatory roles. To make this even more confusing the roles they have are dependent on the cell and its surrounding environment). Increased stress reduces proper regulation of the immune system leading to increased and unregulated inflammation. This inflammatory activity in the brain may contribute to cognitive impairment. For example, an overwhelming immune response known as “cytokine storm” can allow inflammatory mediators, like cytokines and chemokines into the brain and can have long-lasting consequences on the brain 3,4. For example, research in laboratory mice infected with SARS-CoV1 have reported increased cytokines in the CNS and neuron cell death (Netland et al., 2008). Increased cytokines throughout the body increase immune cell infiltration into the CNS, and their entry disrupts normal neurological function 6. In humans, coronavirus infection (SARS-CoV1), caused central nervous system damage 7. Long term consequences of exposure to the SARS-CoV1 virus include symptoms of post-traumatic stress disorder (PTSD), depression, pain disorder, panic disorder and obsessive compulsive disorder 8.
Although there is currently no evidence that COVID-19 can cause degenerative neurological disease (Troyer et al., 2020), it is important to remember that it is a new disease in the human population. Currently, consequences of COVID-19 include loss of smell and taste 10.
Effects of control strategies on mental health and what to expect
The strategies employed to reduce the spread of COVID-19 are unparalleled in the experience of most contemporary Americans. Humans are social animals and as such, it is not easy to practice physical distancing. Therefore these experiences likely contribute to increased stress during the pandemic. In fact, previous populations dealing with coronavirus outbreaks have reported high incidence of psychological distress 3. Consequently, you can expect to feel increased anxiety. This is because we worry about our own health and the health of close relatives. We also worry about the health of the entire population of our country and all of humanity. The anxiety is worsened by feelings of inadequacy in being able to ensure the safety of the family. Many people, even those not living by themselves, might feel lonely which increases anxiety.
An increased sense of fear is also normal. This fear comes from increased scrutiny of our own behaviors and the behavior of others. Initially, the pandemic fear was also caused by difficulty in securing groceries.
An important source of frustration is the temporal aspect of a pandemic. We are easily frustrated when we don’t know how long things will remain in the current (undesirable) condition. This may lead to lose one’s temper, and makes it easier to feel anger towards the behavior of others, especially when you believe they are putting your security at risk. All of these contribute to an increased desire to use alcohol or other drugs as a coping mechanisms.
Finally, health care professionals aiding COVID-19 patients are at increased risk of post-traumatic stress disorder (Lee et al., 2018). These personnel must manage the responsibilities of their jobs along with all of the aforementioned stressors. We will continue to learn about the consequences of infection for a long time. It is important to consider that people may develop neurological disease as a consequence of COVID-19. This means that we may need to mobilize mental health personnel to affected areas and monitor people, including the health of the professionals currently addressing the physical symptoms of the pandemic. This is likely going to require a long term commitment and resources.
Recommendations 12
Physical distancing, isolation and quarantines are likely to impact our mental health. What actions can we take to reduce the impact of these strategies?
1) Be aware and manage expectations
All of the strategies we are currently using to “flatten the curve” are likely to have psychological consequences. These are stressful times. Be aware that you are stressed. This is normal.
You will likely be less productive when trying to work from home. This is normal and to be expected. Take it easy on yourself and the goals you set. You will have to learn to re-evaluate your productivity under new circumstances.
2) Maintain your daily routines
Identify parts of your daily routine that are changing. Acknowledge that things have changed, but don’t give yourself a hard time. Everything has changed. It’s natural that some of the daily routines are changed.
Maintain your routine as much as possible. The previous point aside, if a particular part of your routine doesn’t need to change, then work as hard as possible to maintain that part of the routine in your day.
-
- If you usually workout in the mornings or afternoons, before work or after work, then continue to do that.
- Wake up at the same time you used to when you were traveling to a workplace.
- Shower, shave, clean your teeth on your regular schedule.
- Get dressed and prepared the same way as if you were commuting to your workplace.
3) Develop good sleep practices. Sleep is important to proper emotional responses 13. Recommendations 14 to enhance your sleep hygiene include:
Increase your exposure to sunlight. Indirect sunlight is effective so open up your blinders or curtains.
Reduce caffeine and alcohol. Especially 2-3 hours before bed.
Exercise is great and helps with sleep. But you should not hit the gym or exercise right before going to bed. Also, don’t put any stress on your workout. Exercise helps, stress does not.
Don’t keep a clock in your bedroom, since you will feel tempted to check it in the middle of the night.
Do not use your bed for anything other than sleep or sex. No eating, reading, working or talking on the phone while in bed.
Always go to bed at the same time. Always get up from bed at the same time.
Develop a sleep routine and strategy during your waking hours. Do not try to figure out how you are going to fall asleep when you are in bed. This will cause stress and reduce the chance you will fall asleep.
You should only take sleep aid drugs that may be “habit forming” under medical advice and supervision. These drugs may be useful if taken under these conditions and relatively short periods of time. They are also likely to be appropriate if a mental health professional has previously diagnosed other mental disorders.
4) Improve awareness of yourself.
Breathe: focus on your breath. How do you breathe? How long does it take you to inhale and exhale? Do you breathe differently under different circumstances? Focusing on your breath will help you become more self-aware.
Take your body temperature: While it has been generally acknowledged that the temperature of an average human is 98.6 0F (37 0C) it has recently been reported that the “average” body temperature changes over time (Protsiv et al., 2020). Changes like improved hygiene, better diets and awareness of germ theory have contributed to reducing the “average” body temperature. What is your average temperature? Does your body temperature change with activities you are carrying out or time of day?
Keep a Journal: Consider keeping a journal while starting new projects at home to monitor your thoughts and reactions to new projects. Especially notice differences between the methods you use and those of collaborators or teachers.
5) Be compassionate.
First and foremost, be compassionate towards yourself. It is hard to acknowledge stress, but be aware that you are feeling it. Be aware of your complaints to others. It is normal to complain, but be aware that you are doing it. Understand the purpose of your complaint and the basis of your arguments.
Be compassionate towards others. Everyone is stressed. They might be lacking sleep, feel lonely, anxious and/or depressed. Not everyone will have the best strategies to deal with the stress of the situation. Be understanding of others view-points, even when you don’t share them. You can share your best resources to reduce stress with others.
6) Stay in touch with family and friends. Remember the strategy is physical distancing, not social distancing. You can take advantage of all of methods of communication available to us in the 21st century. Reach out to those you love and share with them your feelings, including your frustrations and personal victories.
7) Understand the current situation, the risks to yourself and to others.
Identify and use credible sources of information.
Stay in the present. There is a lot of information (including this page) that tries to contextualize our current situation.
-
- Using historical analogies or trying to borrow observational data from other events that have caused people to physically distance is useful.
- It is important to understand that the current situation presents unique challenges and will require unique solutions.
- Communicate with family, friends, collaborators and ask them for resources they believe may be able to provide reliable information.
Discuss similarities and differences of the measures being taken in your communities. Share the best ideas and try to enhance our response as a society.
Communicate your ideas about COVID-19. Talk to people you trust about your attitudes towards those that are infected. Discuss possible sources of stigma. Challenge ideas you disagree with in a respectful manner.
Be happy, stay healthy. Happiness and a healthy lifestyle will boost your immune system.
Acknowledgements:
We would like to thank Yasmin Diodonet, LCPC, for her revision of this article.
Bibliography:
- Chu, D. K. et al. Physical distancing, face masks, and eye protection to prevent person-to-person transmission of SARS-CoV-2 and COVID-19: a systematic review and meta-analysis. Lancet (London, England) 6736, 1–15 (2020).
- Zhou, F. et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet 6736, 1–9 (2020).
- Kim, H. C., Yoo, S. Y., Lee, B. H., Lee, S. H. & Shin, H. S. Psychiatric findings in suspected and confirmed middle east respiratory syndrome patients quarantined in hospital: A retrospective chart analysis. Psychiatry Investig. 15, 355–360 (2018).
- Mak, I. W. C., Chu, C. M., Pan, P. C., Yiu, M. G. C. & Chan, V. L. Long-term psychiatric morbidities among SARS survivors. Gen. Hosp. Psychiatry 31, 318–326 (2009).
- Netland, J., Meyerholz, D. K., Moore, S., Cassell, M. & Perlman, S. Severe Acute Respiratory Syndrome Coronavirus Infection Causes Neuronal Death in the Absence of Encephalitis in Mice Transgenic for Human ACE2. J. Virol. 82, 7264–7275 (2008).
- Dantzer, R. Neuroimmune interactions: From the brain to the immune system and vice versa. Physiol. Rev. 98, 477–504 (2018).
- Wu, Y. et al. Nervous system involvement after infection with COVID-19 and other coronaviruses. Brain. Behav. Immun. 1–5 (2020). doi:10.1016/j.bbi.2020.03.031
- Lam, M. H. B. et al. Mental morbidities and chronic fatigue in severe acute respiratory syndrome survivors long-term follow-up. Arch. Intern. Med. 169, 2142–2147 (2009).
- Klopfenstein, T. et al. Features of anosmia in COVID-19. Med. Mal. Infect. 4–7 (2020). doi:10.1016/j.medmal.2020.04.006
- Troyer, E. A., Kohn, J. N. & Hong, S. Are we facing a crashing wave of neuropsychiatric sequelae of COVID-19? Neuropsychiatric symptoms and potential immunologic mechanisms. Brain. Behav. Immun. 0–1 (2020). doi:10.1016/j.bbi.2020.04.027
- Vorspan, F., Mehtelli, W., Dupuy, G., Bloch, V. & Lépine, J. P. Anxiety and Substance Use Disorders: Co-occurrence and Clinical Issues. Curr. Psychiatry Rep. 17, (2015).
- Lee, S. M., Kang, W. S., Cho, A. R., Kim, T. & Park, J. K. Psychological impact of the 2015 MERS outbreak on hospital workers and quarantined hemodialysis patients. Compr. Psychiatry 87, 123–127 (2018).
- Dickerson, D. Seven tips to manage your mental health and well-being during the COVID-19 outbreak. Nature (2020). doi:10.1038/d41586-020-00933-5
- Simon, E. Ben et al. Losing neutrality: The neural basis of impaired emotional control without sleep. J. Neurosci. 35, 13194–13205 (2015).
- Altena, E. et al. Dealing with sleep problems during home confinement due to the COVID-19 outbreak: practical recommendations from a task force of the European CBT-I Academy. J. Sleep Res. 1–7 (2020). doi:10.1111/jsr.13052
- Protsiv, M., Ley, C., Lankester, J., Hastie, T. & Parsonnet, J. Decreasing human body temperature in the United States since the industrial revolution. Elife 9, 1–11 (2020).
N
Nucleic Acids
These are cellular components or building blocks. Cells (and viruses) used these molecules to transmit information.
Nucleic acids are long chains (DNA or RNA strands) store and carry the information to make a new cell (or virus).
Nucleic acids are composed of nucleotides, like the adenine shown above. Nucleotides are able to store and transfer energy to other cellular building blocks or alter their structure. These nucleotides (ATP or GTP) function as the “energy currency” of the cell.
The world is a different place (through the eyes of the human)
I have been recently thinking about the differences we have when viewing the world. But I don’t mean large philosophical differences. What I mean is my eyes let me see certain things and not others. My buddy Steven is a human, not his fault, that’s just the way he was born. Apparently his eyes are somewhat different than mine. Fundamentally our eyes work the same way. They take up reflected light from an object and special cells help us paint a picture of the world.
Special cells in our eyes called cone cells collect color information from the environment. Dogs have two types of cone cells that allow us to see things that are blue and things that are yellow. Humans have three of these cone-cells in their eyes which means that when my buddy and I go to the beach he sees things a little differently than me!

There is another important difference between my eyes and Steven’s. There are a second set of special cells in the eyes of all mammals. Cells called rod photoreceptors, which both dogs and humans have, act as receptors for light. There is a special type of protein in these cells called rhodopsin. Rhodopsin is the protein that captures light.
That is where similarities between dogs and humans come to an end. In my eyes rhodopsin absorbs dimmer light, which means light that has less energy. What this means in practical terms is that my eyes can pick up details in the dark. I wouldn’t call it night vision, but my eyes are better at distinguishing details in light humans may consider dim.
Dogs have a second trick to help us see better in the dark. There is a special structure in our eyes composed of a special protein. It works by reflecting light the same way as reflectors on a bike work. When light hits a reflector the light bounces off and scatters in many directions (including the eyes of a cars’ driver) allowing them to see the bicycle. In a similar manner the light that bounces off of the “tepetum lucidum”, that special structure, of my eye allows the rod photoreceptors to pick up light it might have otherwise missed. This allows me to get a more complete picture of my environment even when there is very little light.
Unfortunately, in very intense light something called photo-bleaching happens and the protein that absorbs light is depleted. This means that I am “blinded-by-the-light” temporarily. After some time my eyes will make more protein and I will be able to see again, but my eyes take twice as long as a human eye to make protein. I have asked Steven not to throw a ball at me when we come in from a walk, but he always seems very eager to play!
Some humans have been interested in how dogs are able to see and perceive the world and have carried out experiments using videos. Unfortunately, it is difficult for humans to understand that a dog’s eye is very sensitive to movement. This means that I don’t see a video in the same way that humans do. Notice how in the video below the clip on the right isn’t as smooth as the one on the left. The right panel is how I see programming on T.V. This means that my researcher friends have to be very careful in interpreting the data from their experiments, since they shouldn’t assume that dogs and humans see the same things.
There are many differences between humans and dogs and how we each see the world. There are also many differences between how different breeds of dog see the world. Over 500 breeds exist, and that’s not even counting mixed-breeds such as myself. Here are a couple of my friends at the park so you can see some of the differences in size and physical activity. The panel on the right shows you how I see other dogs!
There are important differences in how we each see the world based on how far apart our eyes are (think about a wide-eyed Chihuahua and a broad-faced pug). Dogs with longer snouts tend to have their eyes closer together and do better in motion perception tests. This means that humans relate more with how those dogs view the world. Still, it is important to remember that not all dogs will see the world in the same way.
Steven was recently working on something. It is amazing how resilient people can be during hard times. Also, he was commenting on how people adapt to their circumstances and make the best of them. I guess he must have also realized that although dogs don’t see the world the same way as humans our adaptations allow dogs to work well with humans. If he can learn how important it is to recognize and value the differences between each other, perhaps there is hope. Perhaps we will all be able to understand the world is a different place depending on your perspective.
This was fun! Maybe some other time I’ll tell you about elephants or ducks or maybe some more about dogs. In the meantime, if you would like to know more about how dogs see the world check this out. It’s time for my nap!
Bibliography:
Byosiere, S. E., Chouinard, P. A., Howell, T. J., & Bennett, P. C. (2018). What do dogs (Canis familiaris) see? A review of vision in dogs and implications for cognition research. Psychonomic Bulletin and Review, 25(5), 1798–1813. https://doi.org/10.3758/s13423-017-1404-7
SARS-CoV2 and development of COVID-19

The SARS-CoV2 virus causes COVID-19
An RNA virus enters a cell and uses normal cellular processes to make copies of itself. SARS-CoV2 has this replication cycle. As SARS-CoV2 exits the cell by exocytosis it doesn’t damage the cell.
The corona virus SARS-CoV2 is the agent responsible for causing the COVID-19 respiratory disease. Viruses are small bundles of nucleic acids, covered by protein to protect them from environmental damage. If the virus is able to enter a proper host cell, this bundle has a set of instructions that allows the virus to use normal processes in the host cell to produce copies of itself. This virus was initially discovered and described in December, 2019 in China and the name COVID-19 is derived from “Corona Virus Disease 2019”. This is the replication cycle of a virus like SARS-CoV2 in a human cell:
When the world discovers a virus, scientific and health authorities obtain the following information: origin of virus, genomic sequence (genome), and transmission method, effectiveness of transmission, symptoms and disease progression. This strategy allows health systems to prepare the tools necessary to control infection in an individual, reduce the number of infections in the population, predict future epidemics and avoid pandemics.
The SARS-CoV2 is related to SARS-CoV1, responsible for the 2002-2003 SARS epidemic. There is no evidence this virus was developed as a biological weapon.
The SARS-CoV2 appears to be related to SARS-CoV1 that caused the 2002-2003 SARS epidemic, that was largely restricted to South East Asia (Gorbalenya et al., 2020). Both of these viruses are part of a large group of viruses that infect many mammals and in humans may cause respiratory diseases (such as the common cold). Corona viruses cause up to one third of all colds (Maier, Bickerton, & Britton, 2015). In the wild bats are the natural reservoirs for both SARS-CoV1 and SARS-CoV2 (Benvenuto et al., 2020).
COVID-19 is a zoonotic disease
Occasionally, a viruses have a small changes to their genetic sequence (mutation) which may alter its infectivity and allow it to infect humans. Housing bats and other wild animals close to humans causes transmission of a disease from an animal to a human, an event known as zoonosis and the disease is referred to as a zoonotic disease. Occasionally there is an intermediate animal that transmits disease to humans, such as a domesticated animal. This is the case for camels and the coronavirus responsible for the Middle Eastern Respiratory Syndrome. Domestic animals can’t transmit the SARS-CoV2 to humans. SARS-CoV2 can infect domestic cats and transmit to other cats. Therefore, cats should be considered reservoirs for the virus (Shi et al., 2020), although there is no evidence that cats can infect humans.
The SARS-CoV2, which causes COVID-19 is not transmitted from domestic animals to humans.
It is very rare that viruses evolved to infect another animal, such as bats or cows, infect humans. The virus has proteins on its surface that have evolved to infect specific species. Bats have tolerant immune systems which allow the virus to replicate inside their cells without causing the bat harm. The virus can remain in these bat populations for a long time (hundreds or thousands of years), acquiring mutations. Eventually, and through a random process, enough mutations accumulate to allow the virus to infect cells in another species of animal (Parrish et al., 2008). It is important to determine the source of the virus. This helps us understand how different the virus that infects humans is from its progenitor found in wild life. That information is useful in tracking disease and predicting future outbreaks.
genomic sequences yield important information
The rate at which viruses acquire mutations is important because it can tell us the origin of the virus (Benvenuto et al., 2020). Nextstrain.org has a weekly updated graph containing information that shows how small molecular changes allow us to track the spread of the virus. Knowing changes to the sequence allow scientists to develop drugs that inhibit infection or develop an effective vaccine. The following figure shows different parts of the viral “life-cycle” and therapeutic opportunities being explored (Smith, Bushek, & Prosser, 2020).
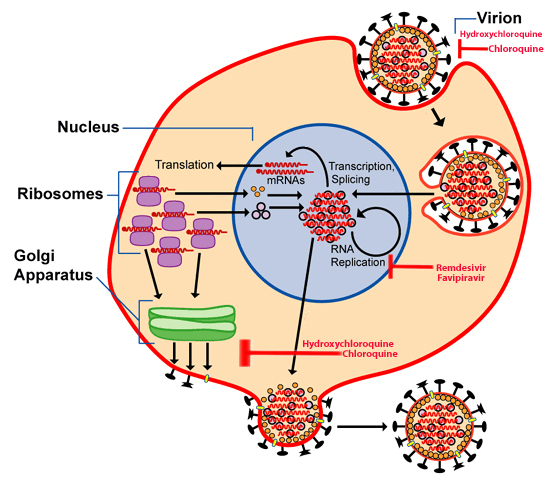
Hydroxychloroquine and chloroquine are drugs that inhibit the virus from entering or exiting an infected cell. Remdesivir and favipiravir interrupt the replication of the long nucleic acid chains viruses need to create copies. All of these therapies are experimental and should only be used under medical supervision.
The entire sequence of SARS-CoV2 genome has been determined and published. It is freely available for examination. The structure of the “spike” protein is determined using the genomic sequence of the virus. Viruses enter the cell using this protein as a kind of molecular “key”.
When this protein on the virus comes into contact with its “door” on the surface of a host cell, it is able to enter the cell and begin the process of transforming the cell into a replication system for the virus. These viral replicas exit the cell (sometimes causing damage) and go on to infect other cells. Coronaviruses, including SARS-CoV1 and SARS-CoV2, exit the cell by a process called exocytosis that does not damage the cell. The ACE-2 protein acts as a doorway which allows the SARS-CoV2 to enter human cells. This protein is found on many cells in our bodies (lungs, GI tract, heart). This is precisely the same protein that SARS-CoV1 uses to enter human cells (Wang et al., 2020).
Viruses cause potent immune responses
Entry of the virus into the cell causes its transformation into a virus replication machine. Therefore the infected cell is no longer able to carry out its normal function. Cells in blood vessels or airways are no longer able to efficiently move blood or gases (oxygen or carbon dioxide) throughout the body. These infected cells signal the immune system that they contain a foreign nucleic acid.
Infected cells also signal the immune system that they contain a foreign nucleic acid. After sending an “infected” signal to the immune system, cells attempt to stop viral replication.
Some corona viruses have an interesting mechanism that allows them to avoid detection by the host organism. Proteins remaining in the cell (but not packaged into new virus) can cause a fusion of the infected cells with surrounding cells. These fused cells are not able to carry out normal functions either. This interesting mechanism allows the virus to replicate without alerting immune cells to its presence (Maier et al., 2015).
After sending an “infected” signal to the immune system, cells attempt to stop viral replication. Infected cells and tissues sometimes undergo cell death (via a process called apoptosis) further decreasing their functions. If cells fail to die in an orderly fashion it results in tissue damage and causes cells in the immune system increase inflammation and swelling (edema).
All of these responses result in a general loss of the function of the infected cells. The tissues made up of these cells (in airway this leads to difficulty breathing or dyspnea). In certain individuals, such as the elderly and those with other diseases (cardiovascular, lung and kidney disease and those with diabetes), this inflammatory condition is more likely to spin out of control causing severe and critical COVID-19. As the inflammation continues, airway tissue and organs fill up with liquid and lose blood circulation.
In certain individuals, such as the elderly and those with other diseases an inflammatory condition spins out of control causing severe and critical disease. If lungs, heart and kidneys fail, the rest of the body (including the brain) is no longer able to carry out its normal functions.
The cells that make up the organs are incapable of excreting the waste normally generated by cells. They are also less capable of obtaining oxygen and nutrients. This causes organ failure. If lungs, heart and kidneys fail, the rest of the body (including the brain) is no longer able to carry out its normal functions. The person slips into a fatal coma and dies. This is the typical progression for a portion of severe and critical patients with COVID-19 (Huang et al., 2020).
Recommendations
We have discussed SARS-CoV2 and the development of COVID-19. This disease has become a global pandemic. Health authorities in the United States recommend the following steps to restrict the spread of SARS-CoV2 and avoid overwhelming hospitals. For asymptomatic individuals:
- Develop/maintain a healthy life-style with focus on exercising and a balanced diet
- Maintain social distancing practices in public places
- Wash your hands frequently
- Cover your mouth before sneezing or coughing
- Stay informed. You can use the links provided in the resources section of this document.
For people with cold symptoms (fever, cough, sore-throat, etc.):
- Stay at home
- Take and keep records of your temperature
- Use over the counter medications to control fever
- Call your physician or local hospital if you have a fever that is not controlled by medications or the cough causes fatigue.
If you have symptoms of pneumonia (difficulty breathing or continuous cough) or have been exposed to a person who is positive for COVID-19:
- Call your physician or hospital
- Call family or friends you have seen in the previous five days and ask them to stay at home and monitor their health.
This page has additional resources. You can also get the information in this article in a summarized form here.
Bibliography:
Benvenuto, D., Giovanetti, M., Salemi, M., Prosperi, M., De Flora, C., Junior Alcantara, L. C., … Ciccozzi, M. (2020). The global spread of 2019-nCoV: a molecular evolutionary analysis. Pathogens and Global Health, 00(00), 1–4. https://doi.org/10.1080/20477724.2020.1725339
Gorbalenya, A. E., Baker, S. C., Baric, R. S., de Groot, R. J., Drosten, C., Gulyaeva, A. A., … Ziebuhr, J. (2020). The species Severe acute respiratory syndrome-related coronavirus: classifying 2019-nCoV and naming it SARS-CoV-2. Nature Microbiology, 5(4), 536–544. https://doi.org/10.1038/s41564-020-0695-z
Huang, C., Wang, Y., Li, X., Ren, L., Zhao, J., Hu, Y., … Cao, B. (2020). Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. The Lancet, 395(10223), 497–506. https://doi.org/10.1016/S0140-6736(20)30183-5
Maier, H. J., Bickerton, E., & Britton, P. (2015). Coronaviruses: Methods and protocols. Coronaviruses: Methods and Protocols, 1282(1), 1–282. https://doi.org/10.1007/978-1-4939-2438-7
Parrish, C. R., Holmes, E. C., Morens, D. M., Park, E.-C., Burke, D. S., Calisher, C. H., … Daszak, P. (2008). Cross-Species Virus Transmission and the Emergence of New Epidemic Diseases. Microbiology and Molecular Biology Reviews, 72(3), 457–470. https://doi.org/10.1128/mmbr.00004-08
Shi, J., Wen, Z., Zhong, G., Yang, H., Wang, C., Huang, B., … Bu, Z. (2020). Susceptibility of ferrets, cats, dogs, and other domesticated animals to SARS–coronavirus 2. Science, 7015(April), eabb7015. https://doi.org/10.1126/science.abb7015
Smith, T., Bushek, J., & Prosser, T. (2020). COVID-19 Drug Therapy Highlights : Antimicrobials with potential activity against SARS-CoV-2 : Clinical Drug Information, (Cdc), 1–21.
Wang, Q., Zhang, Y., Wu, L., Niu, S., Song, C., Zhang, Z., … Qi, J. (2020). Structural and functional basis of SARS-CoV-2 entry by using human ACE2. Cell, 1–11. https://doi.org/10.1016/j.cell.2020.03.045